- Projects
- Insights
-
Careers

Careers
Ranked a Top Workplace and ENR Top 500 Design Firm, Burns offers opportunities to inspire, create and deliver transformational projects that last generations.
- News + Events
-
About

About
Burns inspires, creates and delivers specialized-engineering solutions for mission-critical facilities.
- Offices
-
What We Do
Discipline
Expertise
Industry-Specific - Projects
- Insights
- Careers
- News + Events
- About
- Offices
"*" indicates required fields
Knowledge is Power: Why Legacy Electric Infrastructure in Healthcare Facilities Demands Strategic Updating
Upgrading electrical infrastructure in healthcare facilities is a complex task. Because these facilities often operate 24/7, downtime during renovation or construction must be minimal, and the work must be phased. Space is always constrained because electrical rooms do not generate revenue, even though they are essential for everything in the facility to function. One overlooked weakness can cascade into a catastrophic failure.
Power studies in as-built hospital projects address these realities head-on. They bridge the gap between legacy infrastructure and modern clinical demands. More importantly, they protect the people who depend on these systems—patients, visitors, clinicians, and maintenance staff alike.
Hospital facilities now face three converging forces that make power studies in as-built projects essential: aging equipment, code evolution, and the absence of as-built electrical documentation.
Aging Equipment
The first primary force is aging equipment. Many buildings Burns’ Healthcare Facilities and Infrastructure team works with—especially in New York—are 50 to 70 years old. These facilities are built under different codes with equipment not designed for today’s standards. In many hospitals, core electrical infrastructure, which includes panels, switchboards, and switchgear, was part of the original construction. In some cases, the equipment manufacturers no longer exist. One of these manufacturers, Federal Pacific, is a notable example in the industry. When this type of equipment fails, there are no replacement parts available. Any modification becomes a retrofit, and every fix becomes a band-aid.

Older existing service switchboards require proactive management to prevent failure
In a hospital, the consequences of catastrophic electrical failure are immediate and severe. The Burns team has encountered situations where obsolete electrical equipment was powering infrastructure as critical as operating rooms. Losing power in the middle of a surgical procedure is not an option. Yet without a clear understanding of what exists, how it is connected, and how it behaves under stress, facilities are conducting risky business.
Code Evolution
The second force is code evolution. Hospital campuses are rarely uniform. A single hospital may include buildings constructed from the 1950s through the 1990s, each designed under different versions of the electrical code. While it is all “electrical code,” the requirements are not the same.
When renovations occur, the question becomes unavoidable: which code applies? The original code? The current code? Or specific state requirements? In New York, this complexity is further amplified by the Department of Health’s stringent inspections, conducted on a three-year cycle. Code compliance is not optional, and expectations are far more rigorous than they were in the past.
Over time, the National Electrical Code (NFPA 70) has evolved dramatically from a single 11×7” page many years ago to the 800-page tome that exists today. That evolution reflects a shift from loosely defined guidance to highly enforceable standards driven by life safety. Renovation thresholds now trigger broader compliance obligations, forcing facilities to confront legacy conditions that can no longer be ignored.
Absence of As-Built Electrical Documentation
The third force is the reality of as-built conditions or the absence of them. Designs created 20, 50, or even 70 years ago no longer reflect reality. Rooms have been reconfigured, systems rerouted, equipment replaced, and loads added—often dozens of times. Original drawings are no longer reliable. In many cases, they are meaningless.
That is why developing accurate as-built electrical documentation is foundational. For one facility in New York, this meant creating detailed one-line diagrams that represent the true electrical infrastructure—not every outlet or light fixture, but the complete power distribution system from utility service to downstream panels. These one-line diagrams are the guiding light of electrical operations.
In one facility alone, this meant documenting more than 30 separate electrical services. Each required extensive field surveys, electricians maintaining electrical equipment, documenting breaker sizes, conductor types, and equipment ratings. This level of effort is time-consuming and costly, but without it, facilities are forced to guess during emergencies—and guessing is unacceptable in a hospital environment.
Unfortunately, most hospitals do not have that level of documentation, in turn, depleting the ability of facility personnel to work efficiently and effectively.
The Power of a Power Study
Once accurate as-built conditions exist, power studies become possible. Power studies are not a single analysis, but a structured process built on three interconnected components.
The first is the short-circuit study. Using specialized software, such as SKM, the as-built electrical system is modeled in detail. The study calculates the available fault current at every level of the distribution system under any conditions, from normal operations to catastrophic situations. Electrical equipment must be capable of withstanding these forces long enough for protective devices to operate. If it cannot, the result is equipment damage, fire, or worse.
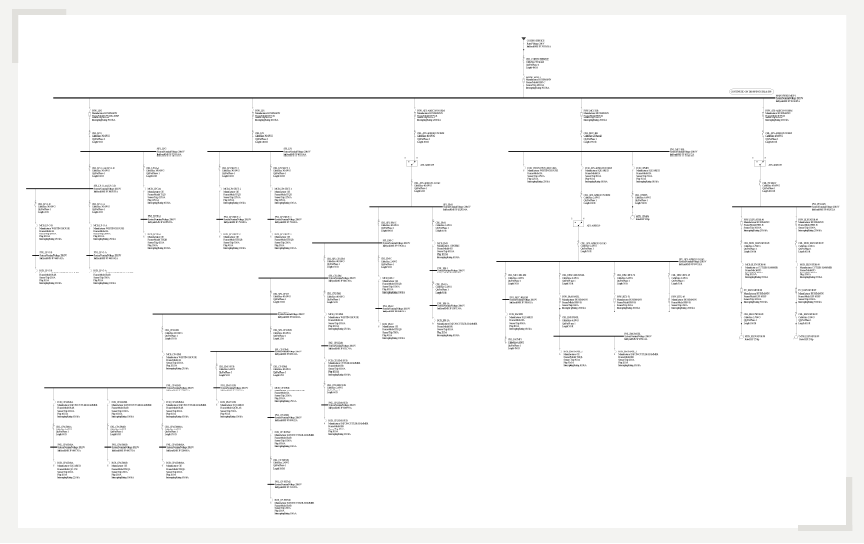
Example of an SKM one-line diagram, graphically illustrating power flow from sources to loads while enabling integrated analyses such as load flow, short circuit, and arc flash studies.
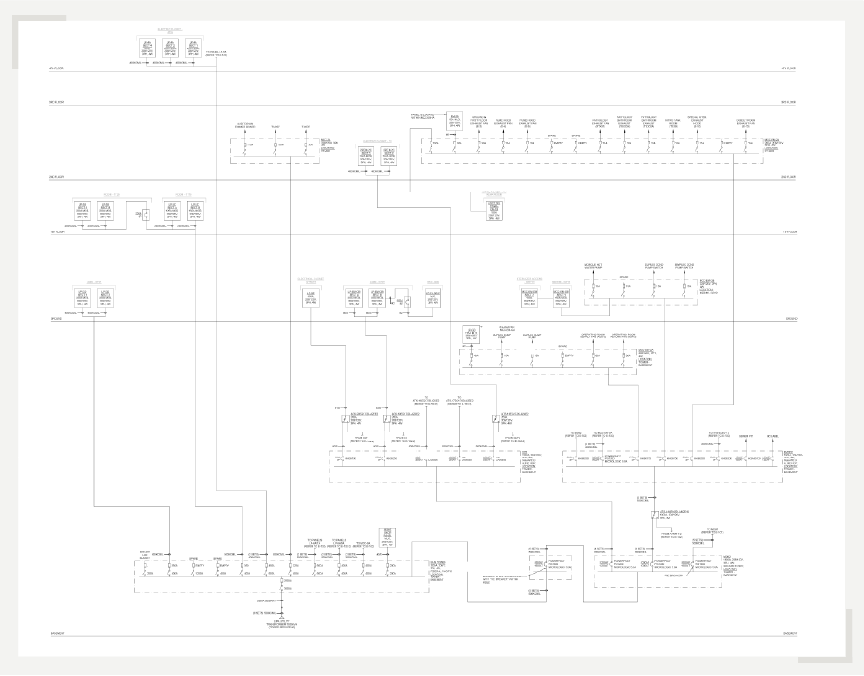
Example of an as-built one-line diagram
The second component is arc flash analysis. A short-circuit event does not just stress equipment; it also releases energy. Arc flash studies calculate how much energy would be released at each piece of equipment and translate that into actionable information. Labels are generated and installed, informing maintenance personnel of the hazard level and the required personal protective equipment.
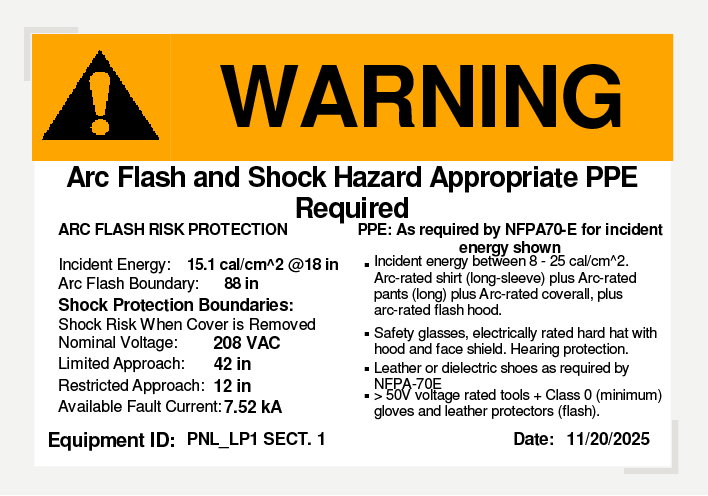
Example of an arc flash label identifying the type of appropriate PPE required
NFPA 70E establishes strict requirements for arc flash protection. In some cases, standard clothing is sufficient. In others, specialized suits, gloves, and face protection are required. In extreme cases, the calculated energy is so high that no PPE is adequate, which means that the equipment cannot be worked on while energized at all.
The third component is a Coordination Study. Coordination Studies provide an understanding of the electrical protection devices within a power system and assists the facilities team in making sure these devices function in a coordinated manner. When the electrical protection devices are coordinated, this minimizes the risk of outages spreading beyond a localized area and causing system-wide outages and shutdowns. Through data collection, system modeling, analysis of fault scenarios, and device setting adjustments, coordination studies provide comprehensive documentation that helps facility managers stay ahead of the game.
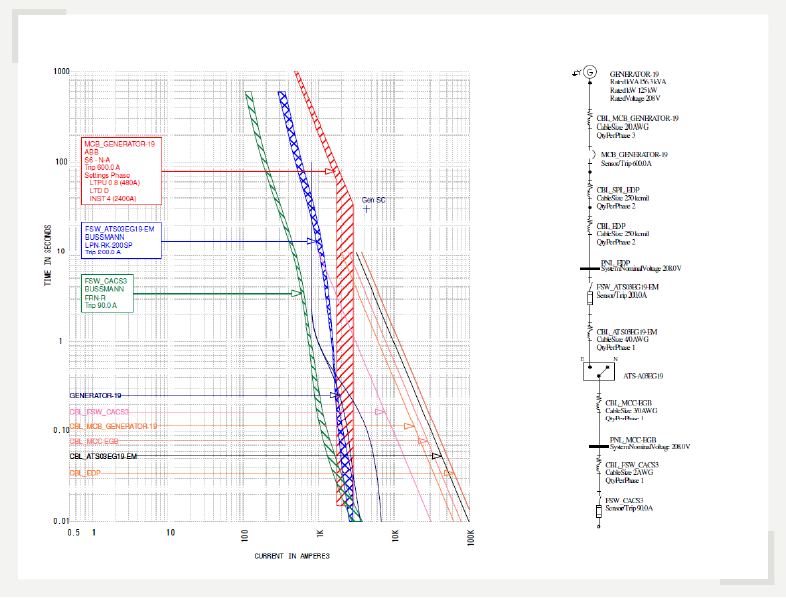
Example of a coordination study diagram
The final product of a power study is a roadmap for improvement— a holistic report of recommendations that identify deficiencies that need to be addressed and how to address them.
Knowledge is Power
Healthcare facilities gain critical knowledge from comprehensive power studies. This enables safe operation, strategic maintenance planning, and swift emergency response. In contrast, without as-built documentation and power studies, maintenance staff face uncertainty about power sources, distribution paths, equipment limits, and safe procedures, increasing operational risk.
The healthcare facilities and infrastructure team at Burns are experts in performing comprehensive power studies. We combine deep insights in code compliance with innovative engineering solutions, establishing an environment of care that supports the healing process and occupant safety.